In this age of amazing medical advances, it seems as though anything broken can be fixed. In my native South Africa, the surgeon Dr. Christiaan Barnard proved that even defective hearts can be replaced when he performed the first heart transplant in 1967.
Despite such innovations, it can surprise many that heart-related conditions remain a leading cause of death and account for a significant percentage of total mortality claims in South Africa and around the world. RGA’s critical illness book in South Africa only reinforces this point – approximately 30% of claims made by males are due to heart-related conditions.
Is it possible that, despite our technical and clinical sophistication, some of us can still die of a broken heart? The answer is, unfortunately, yes.
Broken Hearts and Takotsubo
Broken-heart syndrome (medically known as stress cardiomyopathy or takotsubo) is well-known by clinicians, even if it is less recognized outside the emergency room. This temporary heart condition presents as a heart attack, but without evidence of blockages in the coronary arteries. The patient usually suffers from ballooning or unusual movement in the left ventricular chamber.
While the exact cause is unknown, stress cardiomyopathy is frequently triggered by severe emotional or physical stress and is characterized by intense chest pain and shortness of breath. It could be prompted by emotionally stressful events, such as the death of a loved one, divorce, break-up, or betrayal. 1 Stress cardiomyopathy is generally a temporary disorder managed with supportive therapy, although some patients develop acute complications such as shock and acute heart failure. Interestingly, stress cardiomyopathy is much more commonly experienced by women than by men1, 2 and, though broken-heart syndrome is a short-term phenomenon, the emotional and physical complications can be lasting.
Broken Relationships and Suicide Risk
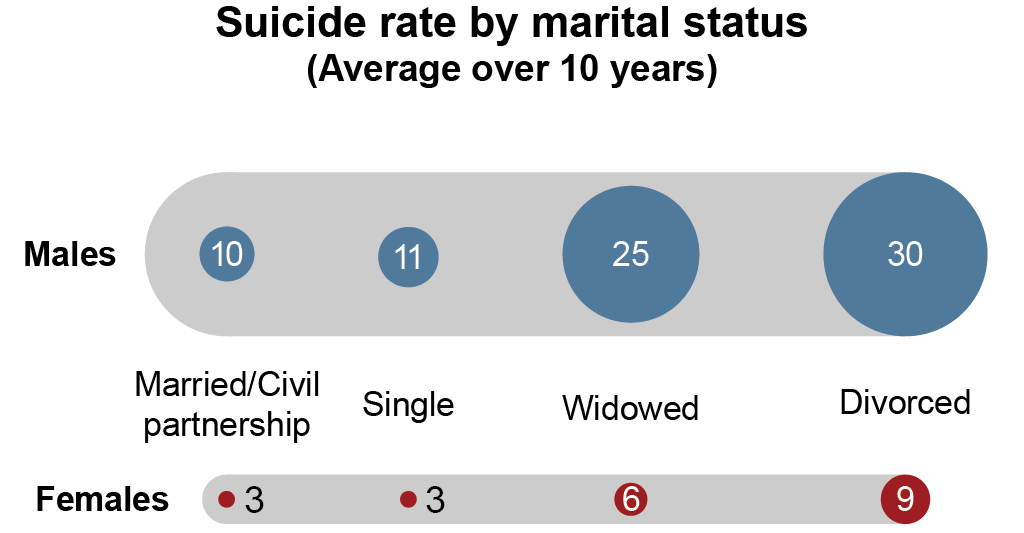
Emotional distress from broken relationships can result in increased mortality risk in more direct ways. In South Africa, roughly 6% of mortality claims can be attributed to suicide, and there is accumulating scientific evidence that divorce and separation could increase suicide risk both within the South African population and populations of other nations. For example, recent studies based on data from the U.K. Office for National Statistics database revealed that the suicide rate of divorced or widowed British individuals was almost three times that of married persons. 3
Researchers3 attributed this increased risk to an individual’s disconnection from domestic relationships and societal supports following the dissolution of a relationship. Some have also hypothesized that some societies’ strong cultural emphasis on achieving a strong and happy marriage could also contribute to feelings of disorientation, shame, guilt, and depression in affected individuals. It is important to note that the effects of divorce on mortality may be:
- Selective. Unhealthy individuals (e.g., individuals with histories of alcohol abuse or depressive episodes) are more likely to practice behaviors that are already associated with higher mortality rates, regardless of divorce.
- Compounding. The stresses of separation and frayed family bonds can contribute to riskier lifestyle choices and the loss of family caregivers during illness.
While divorce is just one example of a broken relationship, the life-changing impact of such a loss, like the dissolution of any important bond, cannot be trivialized.
Happy Hearts and the Role of Insurers
Mortality studies also consistently indicate that social isolation and loneliness can result in another form of heartbreak, and a related rise in all-cause mortality risk. In the 1976 book The Broken Heart: The Consequences of Loneliness, author, researcher, and psychologist James Lynch first suggested that loneliness could be a major hidden contributor to heart disease. He found that even the most transient human contact had marked effects on heart rate and blood pressure. This work spawned an array of scientific articles supporting his thesis and a growing consensus that people cannot afford to take relationships for granted.
Indeed, the long-term impact of loneliness and social isolation has been shown to be comparable to that of excess drinking and smoking.4 This phenomenon is exacerbated by the isolating effects of technology and has been observed among younger generations, not only among the elderly and housebound. Over the years, many pundits have discussed mortality improvement trends and the implications of more people living longer. Fewer have considered that many of the individuals who reach advanced old age watch friends and partners pass away and must live increasingly isolated lives.
Physical activities with groups of people, on the other hand, are associated with a lower risk of heart disease and all-cause mortality and are also directly correlated to a lower risk of developing 13 types of cancers.4 Research from extraordinarily long-lived communities around the globe, called Blue Zones,5 provides evidence that good, supportive relationships among friends, family, and the broader community are important to individuals’ longevity. Longevity is deeply intertwined with certain simple, powerful habits. For example, simply laughing with friends has been found to lower cardiovascular disease risk.6
Underwriters can reference multiple studies indicating that simple lifestyle changes can help prevent heart disease. Factors that are modifiable include poor diet, smoking, hypertension, physical inactivity, and obesity. Loneliness and lack of social engagement could join this list, but because these factors are difficult to quantify, they are not currently used as part of the traditional insurance process. Yet insurers who overlook the emotional well-being and relationships of their customers do so at their own peril. After all, happier hearts often mean healthier policyholders.

