Physical activity has long been associated with improved health and longevity. Even less physically demanding activities such as gardening, do-it-yourself (DIY) projects, and reading have this association.
Mortality studies consistently indicate that over the long term, those who engage in social activities have reduced mortality risk, and social isolation and loneliness increase that risk. Indeed, the long-term impact of loneliness and social isolation has been compared to that of the current obesity crisis (an impact accurately predicted three decades ago), and poor social engagement’s impact shown to be comparable to that of excess drinking and smoking.
Leisure time group physical activities are associated with lower risk of heart disease and all-cause mortality, and is also directly correlated to a lower risk of developing 13 types of cancers. Yet, because loneliness and social engagement are difficult to quantify, they are not currently used as part of the traditional underwriting process.
Introduction
As life expectancies rise, so too does the size of the aged population. According to the United Nations’ “World Population Prospects 2017” report, persons over age 60 represent just over one eighth (13%) of the world’s population. The segment, however, is growing at a rate of about 3% per year, and is projected to reach 1.4 billion by the year 2030.
Physical activity has long been associated with improved health and longevity. Those who complete two to three times the minimum recommended amount of aerobic activity per week are shown to have a 37% lower mortality risk compared to those who report no leisure time physical activity at all.1 Even less physically demanding activities such as gardening, DIY projects, and reading have been associated with lower
levels of mortality.
Clearly all of these factors are important considerations when underwriting an applicant for life, critical illness, and disability insurance. How to utilize this information in risk assessment is a challenging task, but perhaps it not unreasonable for the insurance industry to consider these non-traditional risk factors in the underwriting process.
Loneliness and Social Isolation
Social isolation and loneliness are two increasingly common risk factors for older-age individuals. Causes can include widowhood, feelings of social rejection, living alone, and feeling poorly understood by friends and family.
Social isolation differs from loneliness in that a socially isolated person generally lives alone and has little to no contact or involvement with others. Loneliness generally tends to be a more subjective state, and is described as someone’s perception of their relationships as well as a feeling of lack of connection to others.
Loneliness can influence several risk factors, including diet, smoking habits, and alcohol intake. In a 2016 meta-analysis of 35 articles, loneliness was found to be a risk factor for all-cause mortality in women (HR 1.26), in men (HR 1.44) and for both genders combined (HR 1.22).2 Awang and Osman’s 2017 research into loneliness in older adults noted that the odds of dying at younger ages were about 40% higher for those who report often feeling lonely than those who never did.4
Another meta-analysis examining loneliness and social isolation showed that the increased likelihood of death was 26% for those experiencing loneliness, 29% for social isolation, and 32% for living alone.3 Some studies have shown that increased mortality risk due to loneliness and social isolation is even greater than that from obesity.3 Therefore, insurers may want to consider utilizing this important evidence, if available, for risk stratification purposes.
Loneliness also has an impact on morbidity. A Chinese study found that lonely individuals had a higher incidence of dementia even after adjusting for sociodemographic factors (OR 1.31).5 Other studies found an association with increased vascular resistance, raised blood pressure, increased hypothalamic pituitary adrenocortical activity, and altered immunity.
The data for social isolation differed somewhat. An analysis of data from the UK Biobank study cohort found that social isolation generated increased all-cause mortality (HR 1.73). Socially isolated people were also found to have an increased risk of death from neoplasms (HR 2.06) and diseases of the circulatory system (HR 1.68).7 Day, et al. identified 15 associated genetic variants in the UK Bio bank study that contribute to loneliness and estimated the heritability of loneliness to be 4.2%. Interestingly, they also identified genomic loci that drive engagement in a sports club or gym, a pub or social club, and religious groups.8
Loneliness and social isolation have separately been found to be risk factors for coronary heart disease (CHD) and stroke. A systematic review and meta-analysis of 11 studies by Valtorta, et al. reported that poor social relationships were associated with a 29% increase in CHD incidence and a 32% increase in stroke incidence.9
The seven studies included in Figure 1 show the increased risk of CHD for lonely or socially isolated individuals, with one study even showing a four-fold increase.
Social Engagement
Adults who are socially engaged and have strong social networks have been shown to live longer. In recent decades, however, social interactions have increasingly moved online, which is changing how people interact with each other. As of March 2018, for example, 1.45 billion people were using Facebook daily, according to the company. Unfortunately, the increasing amount of time individuals spend on social media is reducing the amount of time that they would otherwise spend physically socializing in groups and engaging in activities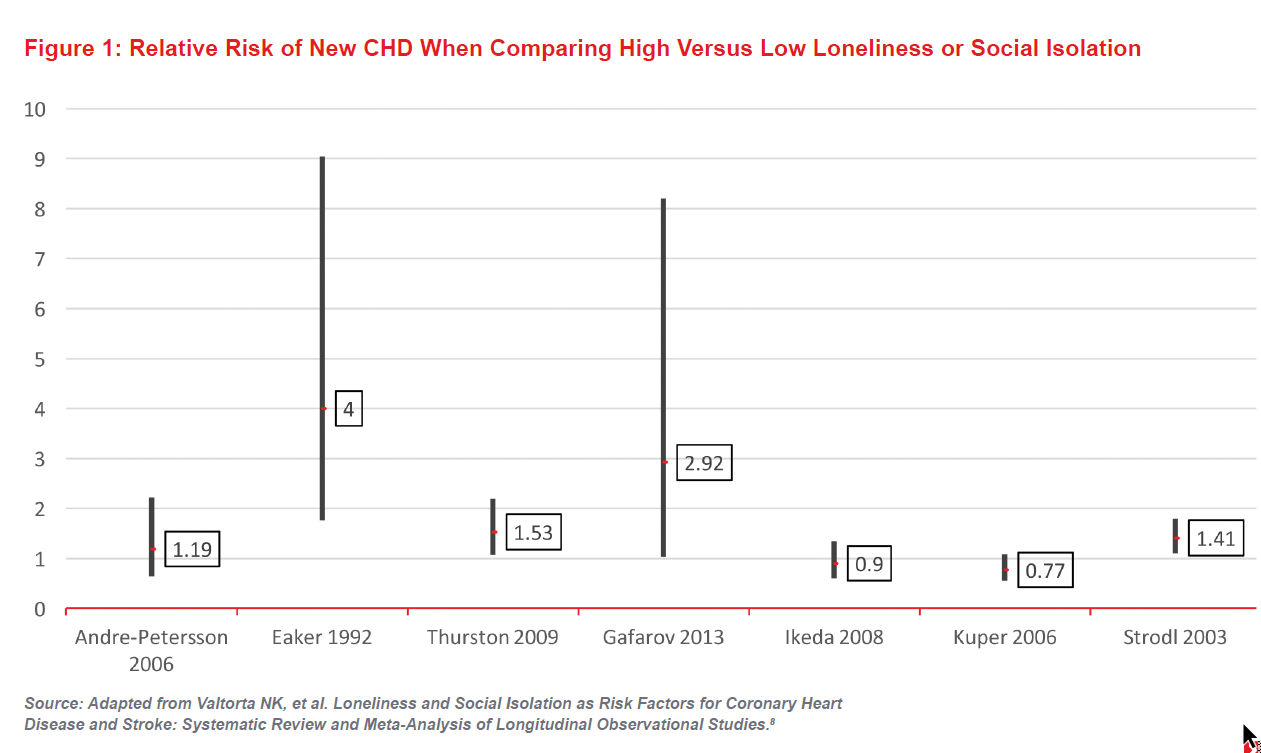
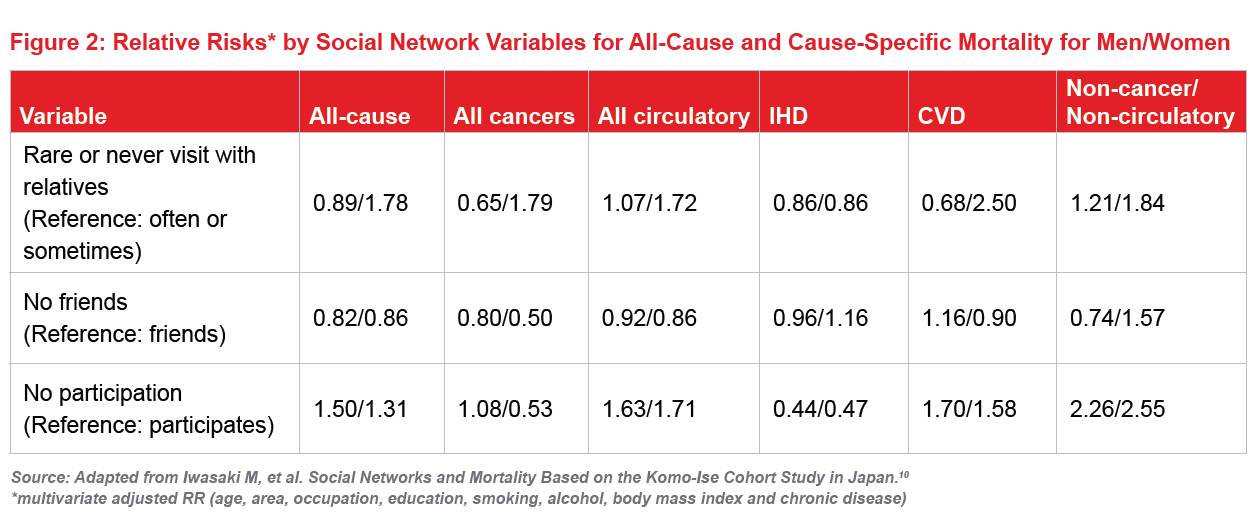
Figure 2 shows the relative risks for all-cause and cause-specific mortality, taken from a study examining the relationship between social networks and mortality in Japan. The study found that single women had significantly higher risk of all-cause and circulatory system disease mortality, and socially isolated women had notably increased risk of cancer mortality. For men, the increased risk of mortality from non-cancer/non circulatory disorders was more than double that of men who participated in activities such as hobbies or club events.10
A meta-analysis by Holt-Lunstad, et al. in 2010 concluded that the positive effect on health of having adequate social networks is comparable with that of stopping smoking, and exceeds the negative impact of other risk factors for mortality such as obesity and physical inactivity.9 The authors suggest that general medical evaluations and screenings could include a section on social well-being and should help to promote improvements of social networks.11 Indeed, perhaps such screenings might be incorporated into wellness programs to improve mortality and morbidity outcomes.
Additionally, the recently released English Longitudinal Study of Ageing (ELSA) showed that those who reported higher enjoyment of life experienced fewer diagnoses of CHD, diabetes, arthritis, stroke or chronic lung disease, and had fewer instances of impaired mobility and impaired ADLs.6
Social and Physical Activity
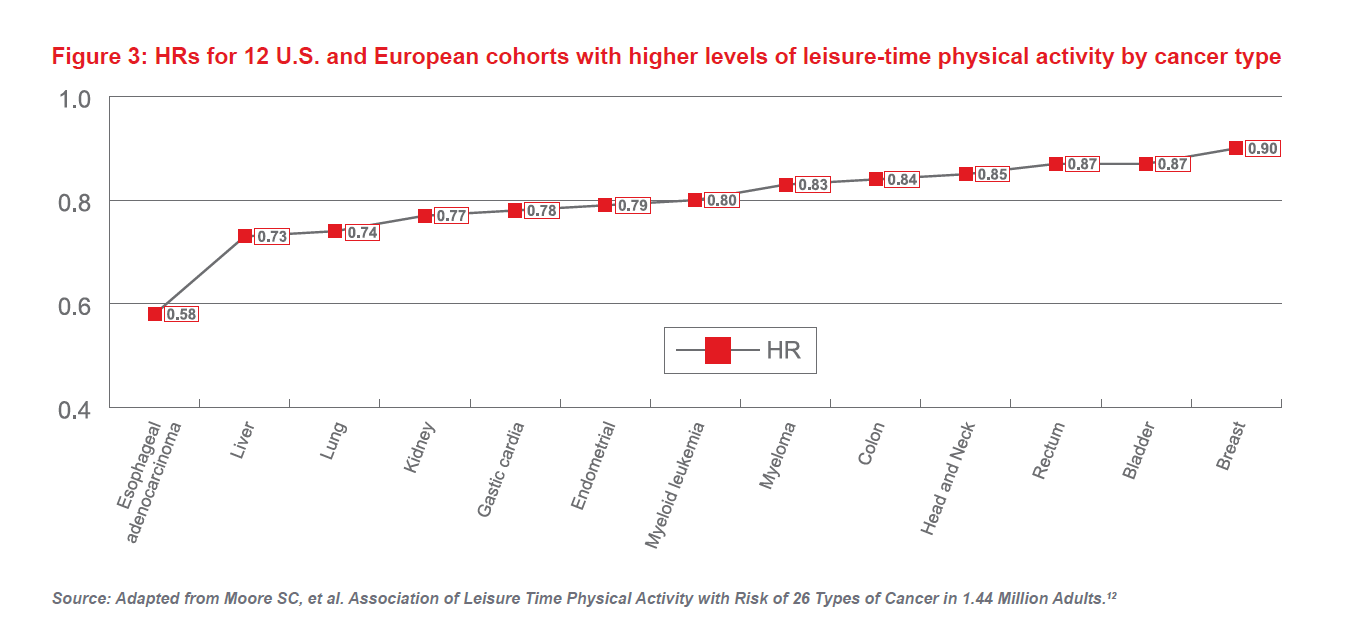
Increased physical activity is known to improve health and longevity, but engagement with others in leisure time physical activities is important as well. Data from 12 U.S. and European cohorts showed that higher activity levels were associated with younger ages, higher educational attainments, lower body mass indexes (BMIs), and lower likelihood of being a smoker. Paradoxically, it was also linked to increased risk of prostate cancer (HR 1.05) and malignant melanoma (HR 1.27). However, the analysis also showed that higher levels of leisure time physical activity was associated with a 7% overall lower risk from all cancers.
Study results presented in Figure 3 show that leisure time physical activity is associated with lower heart disease and all-cause mortality risk and is directly correlated to a lower risk of 13 types of cancers. The most significant correlation was with esophageal adenocarcinoma, with a 42% risk reduction in the physically active participant.
According to the Health Survey for England 2016, an annual survey undertaken by the National Health Service to monitor health trends, 58% of women and 47% of men aged 75 and older reported less than 30 minutes per week of moderate physical activity. This is leaving a large number of older adults at increased mortality risk.13
Owning a pet can increase physical activity. Of all pets, dogs are considered to be the most beneficial for increasing physical activity and reducing cardiovascular risk. Dog ownership is also associated with reducing social isolation and improving perception of well-being. A 2017 Swedish nationwide cohort study on dog ownership and risk of cardiovascular disease and death, for example, showed that dog ownership was associated with a lower risk of all-cause mortality (HR 0.67) and cardiovascular death (HR 0.64) in single-person households.14
Conclusions
Underwriters, claims assessors and pricing actuaries are well aware of the traditional risks presented by raised blood pressure, obesity, high alcohol consumption as examples, but these other lesser-known risk factors discussed in this article are clearly of relevance. The question is: can underwriting applications incorporate them into the risk assessment process, given that they are usually self-reported risks and difficult to quantify in the same way as a blood test? It is worrying that mortality and morbidity risks from lack of social engagement and social isolation have been shown to be higher than from obesity, smoking and excess alcohol. It begs the question if we have been missing other vital mortality risk factors not traditionally used as part of the life assurance application process.

