Since the appearance of SARS-CoV-2 in December 2019, a primary focus has been on the risk of death and overall case fatality rates.
However, as most people infected with the novel coronavirus fortunately do survive, additional attention is now being paid to the potential of clinical consequences and sequelae of the disease after recovery.
Post-recovery fatigue has been previously reported to occur with other infections and is now being reported in some patients who have recovered from COVID-19 disease. This paper intends to review the medical literature regarding post-recovery fatigue associated with certain infections and, specifically, SARS-CoV-2.
Background
Most COVID-19 infections have occurred in the employed age group. The median age of infection has been approximately 50 years, with about 75% of cases in people aged 65 years and younger (Figures 1 and 2). The mortality risk in that age group has been low, but it increases at the older ages (Figure 2).
Source: Adapted from K. Sun, Lancet, doi.org/10.1016/S2589-7500(20)30026-1.
Of those COVID-19 cases in the U.K. requiring hospitalization, 33% are less than 65 years of age, with more than 90% surviving to discharge. Recovery from any illness is dependent on a number of factors that include the pathophysiology of the illness itself, host-specific factors, environmental factors, and the demographics in which the illness occurs. Illness trajectories may vary considerably in populations presenting with a similar condition and determining those who might be considered outliers in terms of expected outcomes is difficult.
Viral illnesses are well recognized as conditions that may be associated with degrees of fatigue. While viral fatigue is usually self-limited, it may persist after the acute phase and result in physical, cognitive, and emotional difficulties that can impact vocational capabilities. Fatigue may be protracted and exacerbated by a lack of proper recognition, unhelpful or inappropriate medical advice, and poor management strategies. Host factors also contribute, including co-morbidity, abnormal illness behavior, and the potential for secondary financial gain.1, 2
The socio-economic consequences of the COVID-19 pandemic have caused employment rates and working conditions to change dramatically, and many workers are experiencing economic difficulty. Additionally, the COVID-19 case load among those approaching retirement is significant.
An understanding of fatigue requires a recognition that the term may be used in a broad range of settings to describe features which include weakness, post-exertional malaise, effort breathlessness, excess somnolence, loss of motivation, lack of interest, poor concentration capacity, and reduced cognition. Disabling fatigue may be a manifestation of psychiatric disorders or may be precipitated by psychiatric illness.2
Fatigue and infection
Significant persistent fatigue is not usually caused by simple illnesses such as upper respiratory infections or gastroenteritis, but it is well described following some systemic infections where concordance between the index illness and fatigue can be established.
Disabling fatigue – persisting for six months or more – may result in impaired daily function. It might satisfy criteria for the chronic fatigue syndrome (CFS), also known as myalgic encephalomyelitis (ME) and systemic exertion intolerance disease (SEID). Current diagnostic criteria are addressed in Part 2 of this document.
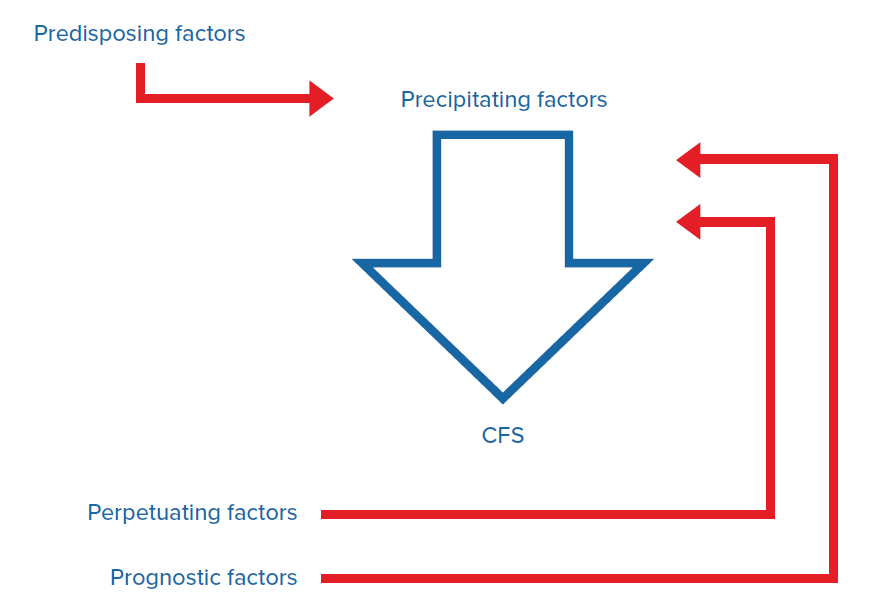
There is no validated diagnostic test or biological marker for CFS; some view it as consequent upon a precipitating event in someone who is predisposed with yet another set of influences causing symptom perpetuation (Figure 3).2, 3 The diagnosis is currently based on clinical criteria that attempt to distinguish it from other conditions that present with fatigue.
Chronic fatigue and the chronic fatigue syndrome are accepted consequences of glandular fever/Epstein-Barr virus (EBV), Q fever, Ross River fever (RRF), brucellosis, Lyme disease, St. Louis encephalitis, severe acute respiratory syndrome (SARS), and Middle East respiratory syndrome (MERS).
Source: Adapted from Lancet, 2006.3
Acute fatigue has been reported in 47% of patients with EBV infection, with fatigue persisting for a median of eight weeks (interquartile range of four to 16 weeks) and chronic fatigue (lasting six months) developing in 9-22% of cases. Acute fatigue was reported in 20% of simple upper respiratory infections. In that setting fatigue lasted for a median of only three weeks (interquartile range of two to four weeks) with no fatigue persisting at six months.4, 5
Hickie followed 253 patients with EBV, Q fever, and RRF selected from laboratory serological reports in Australia. Disabling fatigue, musculoskeletal pain, neurocognitive difficulties, and mood disturbances were reported in 35% at six weeks, 27% at three months, 12% at six months, and 9% at 12 months. Of those fatigued at six months, the majority met 2006 criteria for CFS (Figure 4). The risk for post-viral fatigue was largely determined by illness severity and lower physical fitness at the time of infection. Demographics, premorbid psychiatric illness, and intercurrent psychiatric illness did not have any predictive power for pure fatigue syndromes.6
Source: Adapted from Hickie.6
Mood disorders following viral infection have, however, been shown to be predicted by premorbid psychiatric disorders, emotional personality traits, and social adversity.6, 7
Hulme highlighted those risk factors which were most consistently associated with persistent fatigue after infection. Across all infection types, distress and fatigue at the time of infection onset were risk factors for chronic fatigue, as were the cognitive and behavioral responses to the illness.7
COVID-19 outcomes and fatigue
The long-term outcome in COVID-19 survivors is yet to be clarified. Physicians, epidemiologists, and fatigue interest groups have promoted data from the SARS and MERS outbreaks as evidence to suggest that similar outcomes might be experienced in the COVID-19 context.
The SARS fatigue data has been largely derived from those with a severe acute respiratory distress syndrome (ARDS), including those requiring an intensive care admission. These data, along with data from other ARDS studies, have suggested high rates of chronic disablement.
Despite the fact that COVID-19 is generally a relatively mild illness with low rates of ARDS when compared to SARS, it has been postulated that the high infection rates and high survivorship rates in COVID-19 coupled with the attendant social upheaval and economic disruption might result in significant morbidity and disability.
The experience to date suggests a median time from symptom onset to clinical recovery of about two weeks in mild cases and from three to six weeks in those with severe or critical disease. Recent evidence from the Italian experience has suggested that only 13% of those discharged from hospital care were completely free of symptoms at a mean of 60 days after the acute phase. Residual fatigue was reported in 53% of people (Figure 6).8
Source: Adapted from Carfi et al.8
Warnings of a significant tail should not be discounted, particularly in those who have experienced a life-threatening or protracted illness.
The high prevalence of co-morbidity in COVID-19 populations (hypertension [OR 2.3], diabetes [OR 2.9], chronic obstructive pulmonary disease [OR 5.9], cardiovascular disease [OR 2.9], and cerebrovascular disease [OR 3.8]) might be expected to influence disability outcomes in those deemed to have recovered from the virus itself.9
Non-COVID-19 acute respiratory distress syndrome (ARDS) outcomes
Herridge reported 49% work participation rates at 12 months, rising to 77% at five years, in Canadian ARDS survivors. Reasons for failure to return to work included persistent fatigue, weakness, poor functional status, reduced vitality, work stress, voluntary retirement, and job retraining. Others have reported female gender and home duties as risks. Six-minute walk tests averaged only 66% predicted at 12 months rising to 76% predicted at five years, with limitations including fatigue and weakness (Figure 7). While lung volumes and spirometry had largely normalized at six months, carbon monoxide diffusion capacity was reduced at six months and remained low at 12 months, averaging 70% predicted.10, 11
Source: Adapted from Herridge.11
Moldofsky reported persistent fatigue, depression, muscle weakness, and non-restorative sleep with abnormal sleep physiology in the 10% of SARS cases who had failed to return to work at 20 months. Although poor sleep is essentially universal in CFS, polysomnographic studies have not revealed evidence of a primary sleep disorder.2, 12
Herridge additionally confirmed some degree of permanent disability with reduced quality of life (QOL) in most ARDS survivors. Intensive-care-acquired weakness was a prominent precipitant. Data at five years provided evidence that even young, previously working patients without co-morbidity may not regain their pre-illness functional status or QOL.10, 11, 13
Heterogenous results in lung function have been reported after ARDS. While most young patients without pre-existing lung disease regain normal or near-normal lung mechanics by six months, a mild reduction in gas exchange persists longer term.13
Hopkins demonstrated evidence of impairment in at least one cognitive function in 78% of patients at 12 months post-ARDS discharge, with 48% experiencing decreased speed of mental processing.14
Adhikari identified self-reported depression (41%) and memory deficits (8-20%) at 22 months in ARDS survivors with no demographic or clinical predictors.15
Lam studied the mental health and fatigue status in 233 SARS survivors. Interviews were undertaken at a mean of 41 months post-discharge. The mean age at follow-up was 43 years and 32% were not working. The prevalence of psychiatric illness at the time of SARS diagnosis was about 3%. At follow-up, 42% reported having been given a psychiatric diagnosis at some stage following discharge. Depression, PTSD, somatoform disorders, and panic disorders were the most common diagnoses. Chronic fatigue was present in 40% of those studied, with 27% meeting criteria for CFS. While a continuous improvement in physical symptoms was noted over the first year after diagnosis, the mental health of survivors did not improve in parallel. Chronic fatigue was reported in those with and without psychiatric morbidity.16
In a meta-analysis of the psychiatric and neuropsychiatric presentations and outcomes of novel coronavirus infections, Rogers confirmed a close concordance with infection and post-illness depressed mood, anxiety, impaired memory, insomnia, irritability, fatigue, and traumatic memories of the illness experience.17
Conclusion
While the long-term consequences of COVID-19 are yet to be determined, degrees of post-viral fatigue seem likely, particularly in those who experience manifestations at the severe end of the spectrum. With case numbers not being significant prior to February 2020, insufficient time has elapsed for any true diagnoses of CFS to have been made.
Various sources have warned that persistent and chronic fatigue is an outcome that can be expected, with press reports of “wide-ranging and often bizarre symptoms persisting for weeks and even months after first falling ill.”8
For the small percentage of infected individuals who have required protracted management in an ICU setting, which may have included the need for mechanical ventilation, the potential impact in terms of cognition and physical and mental well-being should not be underestimated. If the SARS experience is repeated in those who have been critically ill with COVID-19, excess morbidity including fatiguing states in the medium and longer term may be anticipated. The degree to which those with minimal or mild symptoms might be expected to develop a fatiguing illness remains unclear.